Breast reconstruction is a physically and emotionally rewarding procedure for a woman who has lost their breast or breasts due to cancer or other conditions.
Breast reconstruction is achieved through several plastic surgery techniques that attempt to restore a breast to near normal shape, appearance and size following mastectomy.
The creation of a new breast can improve self-confidence and quality of life. Although surgery can recreate a relatively natural-looking breast, a reconstructed breast will never look or feel exactly the same as the breast that was removed.
Is a Breast Reconstruction right for you?
Breast reconstruction is a highly individualised procedure. You should do it for yourself, not to fulfil someone else’s desires or to try to fit any sort of ideal image. Breast reconstruction is a good option for you if:
- You have the ability to cope (physically and mentally) with your diagnosis and treatment
- You do not have additional medical conditions or other illnesses that may impair healing
- You have a positive outlook and realistic goals for restoring your breast and body image
- You are not a smoker
- Your BMI is less than 32 and your weight is stable
Breast reconstruction typically involves several procedures performed in multiple stages. It can:
- Begin at the same time as mastectomy (immediate reconstruction), or
- Be delayed until you heal from mastectomy and recover from any additional cancer treatments such as chemotherapy or radiotherapy
Immediate breast reconstruction is most suitable for women:
- With non-invasive cancer
- Having prophylactic mastectomy
- Not expecting postoperative adjuvant radiotherapy
Don’t forget, breast reconstruction may be offered to many patients, but it may not be suitable for everyone. At your consultation, your surgeon will discuss with you:
- Whether breast reconstruction (immediate or delayed) is suitable for you;
- Which type of breast reconstruction is suitable for you;
- Risks associated with each option offered;
- The recovery involved with each option;
- Realistic results that can be expected from breast reconstruction;
- Possible long-term consequences or long-term care commitment required for the reconstruction option offered.
Questions are welcome during the consultation, and the options, results and expectation are explored. It’s important that you feel ready for the emotional adjustment involved in breast reconstruction. It may take some time to accept the results of breast reconstruction. It is also important that you are prepared to undertake the recovery process involved with your procedure.
What is a breast reconstruction?
Breast reconstruction is achieved through several plastic surgery techniques that attempt to restore a breast to near normal shape, appearance and size following mastectomy. Although breast reconstruction can rebuild your breast, the results are highly variable:
- A reconstructed breast will not have the same sensation and feel as the breast it replaces.
- Visible incision lines will always be present on the breast, whether from reconstruction or mastectomy.
- Certain surgical techniques will leave incision lines at the donor site, commonly located in less exposed areas of the body such as the back, abdomen or buttocks.
A note about symmetry: If only one breast is affected, it alone may be reconstructed. In addition, a breast lift, breast reduction or breast augmentation may be recommended for the opposite breast to improve symmetry of the size and position of both breasts.
Risks of Breast Reconstruction
The decision to have breast reconstruction surgery is extremely personal. You’ll have to decide if the benefits will achieve your goals and if the risks and potential complications are acceptable.
Your surgeon will explain in detail the risks associated with surgery. You will be asked to sign consent forms to ensure that you fully understand the procedures you will undergo and any risks or potential complications.
The possible risks of breast reconstruction include, but are not limited to, bleeding, infection, poor healing of incisions, unfavourable scarring and anaesthesia risks. You should also know that:
- Flap surgery includes the risk of partial or complete loss of the flap and a loss of sensation at both the donor and reconstruction site.
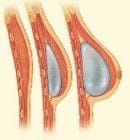
- The use of implants carries the risk of breast firmness (capsular contracture), implant rupture, implant mal-position and implant infection.
- If you require postoperative adjuvant therapy such as chemotherapy and radiotherapy, unexpected complications from breast reconstruction may delay these treatments.
- If you require postoperative radiotherapy, this treatment may damage your reconstruction, altering the shape, volume and appearance of the newly reconstructed breast. Results are often suboptimal and may require revision or repeat reconstruction after you have completed your treatment.
Breast implants do not impair breast health. Careful review of scientific research conducted by independent groups such as the Institute of Medicine has found no proven link between breast implants and autoimmune or other systemic diseases. However, there are rare cancers which are associated with breast implants. To find out more about breast implants, read All About Implants for more information.
Although breast reconstruction surgery can be an effective procedure where the benefits significantly outweigh the risks, like everything in the practice of medicine and surgery, it is not an exact science. The degree of surgical success can be altered by how each individual’s body responds to surgery and healing. Although good results are expected, there is no guarantee. In some situations, it may not be possible to achieve optimal results with a single surgical procedure; revision surgery may be necessary.
Be sure to ask questions: It’s very important to ask questions about your procedure. It’s natural to feel some anxiety, whether it’s excitement or preoperative stress. Don’t be shy about discussing these feelings and any specific concerns with your surgeon or any of our staff members.
Options for Breast Reconstruction
Surgery for your breast reconstruction is performed in a hospital setting, including hospital stay of 5-10 days. Your procedure will require general anaesthesia.
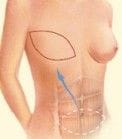
The TRAM/MSTRAM/DIEP Flap
This is where abdominal tissue is transplanted to the chest to recreate the breast mound. TRAM flap stands for Transverse Rectus Abdominus Musculocutaneous flap. A TRAM flap uses donor muscle, fat and skin from a woman’s abdomen to reconstruct the breast. The TRAM flap is based on the deep inferior epigastric artery (DIEA) and veins (DIEV). The MS TRAM is a muscle-sparing TRAM where not all of the rectus abdominus muscle is harvested. The DIEP (deep inferior epigastric perforator) flap is where the rectus muscle is not harvested as part of the flap and the flap only contains the abdominal skin and fat (more details below).
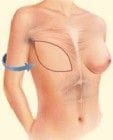
The flap may be transferred to your chest wall in two different ways:
It can remain attached to the original blood supply and then tunnelled up through the chest wall (also known as pedicle flap). Or it can be completely detached with its artery and vein (DIEA and DIEV), transposed to the chest wall and these blood vessels then rejoined to blood vessels behind the ribs using microvascular technique. (This is also known as the free flap).
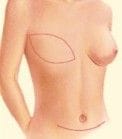
The abdominal tissue is then shaped and inset into the chest wall to create a breast mound.
A variation to the TRAM flap is the DIEP flap. DIEP stands for Deep Inferior Epigastric Perforators. This is where the abdominal tissue (just fat and skin) is taken without the rectus abdominus muscle based on branches of the DIEA and DIEV; whether this is a better alternative than TRAM remains debatable. There are various pros and cons, including different risk profiles of TRAM vs MS TRAM vs DIEP. DIEP flaps are also not suitable for everyone, its viability is heavily dependent on the anatomy of your blood supply and branching pattern of DIEA and DIEV to the abdominal wall - this can be variable between different individuals.
TRAM flap reconstruction can be done as an immediate reconstruction (at the same time as your mastectomy) or delayed reconstruction (after your mastectomy and other treatments such as chemotherapy or radiotherapy). It can also be used to reconstruction for one side (unilateral) or both sides concurrently (bilateral).
Free TRAM flap surgery can take up to 6 hours. Recovery includes hospitalisation for 5-10 days, no driving for up to 4 weeks, and no lifting or straining for 8 weeks. A garment will need to be worn for minimum of 12 weeks postoperatively for both abdominal and breast support. (To find out more about postoperative instructions for this procedure, check out our patient resources page).